
 The lights dim, the audience settle in their seats. The first notes of the accompaniment start… the performer takes a deep breath, and the phrase begins…
The lights dim, the audience settle in their seats. The first notes of the accompaniment start… the performer takes a deep breath, and the phrase begins…
Breathing is something that is fundamental to wind instrumentalists and singers – this is a statement that may seem incredibly obvious. With breathing being something we do passively as we go about our day without being overly aware of it, when it comes to breathing in an optimal way for success on our musical instruments, confusion can quickly set in.
Many teachers get creative with their metaphors and imagery, or use general statements that when put under the microscope, may not actually be giving students the best insight into how their bodies function. They might exclaim “breathe from your belly!” or “support the sound!” These are two of the classic comments about breathing that have been in circulation in music education for decades. They may well produce the desired effect in some students – but statements that lack in physiological reference, or are just not physiologically accurate, have also led to many misconceptions about breathing and the word ‘support.’ This blog will assist in debunking some of these common teaching directives.
“Sing from your Diaphragm!”
 Many teachers talk about the diaphragm – and as the strongest muscle of the respiratory system, it is understandable that it should get some attention – but directing a student to “sing from” it is a little misleading.
Many teachers talk about the diaphragm – and as the strongest muscle of the respiratory system, it is understandable that it should get some attention – but directing a student to “sing from” it is a little misleading.
A survey carried out by Kathleen Spillane in 1989 asked over one hundred singing teachers in North America for their directives to students on the subject of breath support. 93 different directives were returned to her, proving just how hazy and lacking in consensus the subject is as a whole. Many of these mentioned the diaphragm.
One response was “support comes from feeling the diaphragm coming up under the lungs.” Another teacher said that the student should breathe with a “release of the diaphragm muscles” (Spillane, 1989). Now we must debunk several myths here with the following physiological facts:
[accordion multiopen=”true”]
[toggle title=”The diaphragm is only ONE muscle” state=”opened”]
The diaphragm is a complex muscle that divides the torso into two compartments – it acts as a fence between the thorax and the abdomen. More specifically, it separates the heart and lungs from the internal organs – the stomach, intestines, etc.
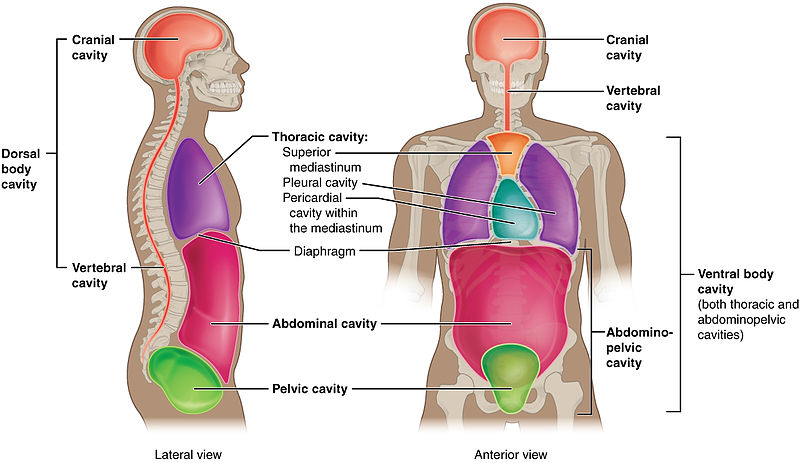
In this diagram, it is the line that separates the thoracic cavity (purple), from the abdominal cavity (pink).
It is a single sheet of long muscle fibres, in a dome-shape that resembles an upside-down bowl. The diaphragm attaches to the bottom of the sternum, lower six ribs and their cartilages, and the first three or four lumbar vertebrae. From here, the broad sheet of muscle extends upwards towards a central tendon (Bunch, 1997; Hixon, 2006; Watson, 2009).
[/toggle]
[accordion multiopen=”true”]
[toggle title=”The diaphragm can only deliver inspiratory force“]
In a study carried out by Watson and Hixon in 1985 they compared what singers thought they were doing as they breathed, to actual respiratory function. One participant talked about how he used his diaphragm “to lift and push air out of the lungs” when he exhaled. This cannot actually happen – because the diaphragm is a muscle capable of delivering inspiratory force only. The strongest of the respiratory muscles, it is always actively engaged in inspiration. It is responsible for at least 60–80% of increased volume in deep inspiration (Bunch, 1997). During quiet breathing (known as ‘tidal volume breathing’), the diaphragm moves approximately 1cm, but during large-volume breathing, the diaphragm can move as much as 10cm (Cloutier, 2007).
It is important to note that this inspiratory force can happen when we control our breathing (i.e. decide to take in a big breath, or we decide to hold our breath for a period of time), or when it is autonomous (for example, when we are asleep and still breathing).
[/toggle]
[accordion multiopen=”true”]
[toggle title=”Our muscles can ONLY contract“]
Another common misconception is the belief that muscles can both expand and contract. In fact, muscles can only contract – producing force in one direction, when the muscle fibres are shortening (Spillane, 1989). When muscles in the respiratory system contract, they create forces that deform the structures of the system, modifying volumes and pressures (Cossette et al., 2010).
Many of the misconceptions with our breathing come from the fact that there are many muscles at play at the same time – the inspiratory and expiratory muscles often contract at the same time as agonist and antagonist muscles, or ‘prime mover’ and ‘opposite force’ (Cossette et al., 2010).
So none of our respiratory muscles are working alone – respiration depends on both passive and active forces applied to the various components of the respiratory system.
[/toggle]
[accordion multiopen=”true”]
[toggle title=”The diaphragm has a poor sensory nerve supply“]
Some people who think they’re using their diaphragm during wind playing will talk about feeling its position moving during a phrase. In actual fact, “the diaphragm is poorly endowed with the types of receptors that would convey such information” (Hixon, 2006). Despite lacking in receptors, we can still feel our diaphragm move, and the displacement of the organs around it.
The fact that we cannot see the diaphragm to ‘show’ students what is happening – as we can with an issue involving their hand position or head angle – only serves to heighten the confusion. What teachers can show students is the outcome of the diaphragm’s contraction: the belly going outwards. When the diaphragm contracts downwards, it pushes the content of the belly down and out, increasing the space in the chest cavity, and lowering the pressure, which causes air to come in. This is inhalation. So despite being difficult to feel, we can see the outcome of its contraction.
Measuring muscle activation in scientific studies can also become problematic, as the tools to do so are sometimes quite invasive. One breathing study talks about the measurements of the diaphragm and intercostal muscle movements as requiring trans-nasal catheters, coupled with electromyographic (EMG) electrodes or EMG needles, which is why the researchers chose to use surface EMG as their measuring tool (Cossette et al., 2010).
Click the play button below to see the surface EMG in action, in this video with researcher Isabelle Cossette:
[/toggle]
[accordion multiopen=”true”]
[toggle title=”If the diaphragm has few receptors, what are we actually feeling then?” state=”opened”]
We can feel the muscles of the abdominal wall, which are muscles of expiration. Unlike the diaphragm, the abdominal muscles contain many sensory nerve endings, so we are well aware when they are active (Watson, 2009). The diaphragm and abdominal wall form opposite surfaces, and sources suggest that it seems likely that when singers report that they are “singing from the diaphragm,” what they really mean is that they are singing using the muscles of the abdominal wall. The diaphragm may just be along for the ride (Hixon, 2006).
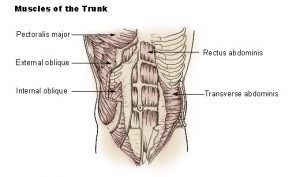 These muscles produce expiratory force only. Put very simply, the four muscles known as “the abdominal muscles” are: the rectus abdominis muscle (on the front of the torso), the external oblique (on the side and front of the lower rib cage wall), the internal oblique (underneath the external), and the transversus abdominis (on the front and side of the abdominal wall). When these muscles contract, they cause the abdominal wall to move inward. These flat muscles act together to raise intra-abdominal pressure, as you might feel when you lift something heavy, or hold your breath. Because of their attachment to the rib cage, the abdominal muscles are also important in stabilizing posture and acting on the spine. (Bunch, 1997).
These muscles produce expiratory force only. Put very simply, the four muscles known as “the abdominal muscles” are: the rectus abdominis muscle (on the front of the torso), the external oblique (on the side and front of the lower rib cage wall), the internal oblique (underneath the external), and the transversus abdominis (on the front and side of the abdominal wall). When these muscles contract, they cause the abdominal wall to move inward. These flat muscles act together to raise intra-abdominal pressure, as you might feel when you lift something heavy, or hold your breath. Because of their attachment to the rib cage, the abdominal muscles are also important in stabilizing posture and acting on the spine. (Bunch, 1997).
[/toggle]
“Breathe from your Belly” “Feel like a Barrel”
 Teachers might tell students to expand as they breathe, or “breathe from the belly.” One of the responses from the already-mentioned breathing directive study was “fill the lungs outward to feel like a barrel – expanding in the back around the waist, as well as the front” (Spillane, 1989).
Teachers might tell students to expand as they breathe, or “breathe from the belly.” One of the responses from the already-mentioned breathing directive study was “fill the lungs outward to feel like a barrel – expanding in the back around the waist, as well as the front” (Spillane, 1989).
It is of course impossible to literally breathe from your belly, or into your belly. This imagery could be used effectively when trying to help a student who might be breathing too shallowly, or raising their shoulders when they breathe; and you want to shift their attention to lower in their bodies. But, it is important that teachers are also aware of the following physiological facts:
[accordion multiopen=”true”]
[toggle title=”The lungs are further up than you might think” state=”opened”]
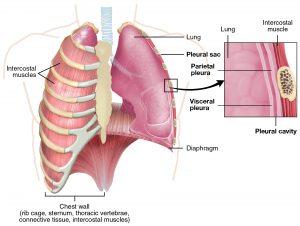 The lungs – our organs of breathing – go as high as the collarbone, and down to the sixth rib. The lungs are served by the pulmonary airways: a collection of flexible tubes that channel air to and from the lungs. Our left lung is slightly smaller, as it has to allow room for the heart. Because of this, the left lung has two lobes, and the right has three. The lungs are made up of a lot of elastic fibres, and behave like stretchable bags. There is a membrane covering the lungs called visceral pleura, and slides against another membrane that covers the inside of the chest wall, called parietal pleura. The two of these membranes essentially hold together because of surface tension, and prevent the lungs from collapsing (Bunch, 1997; Hixon, 2006; Watson, 2009).
The lungs – our organs of breathing – go as high as the collarbone, and down to the sixth rib. The lungs are served by the pulmonary airways: a collection of flexible tubes that channel air to and from the lungs. Our left lung is slightly smaller, as it has to allow room for the heart. Because of this, the left lung has two lobes, and the right has three. The lungs are made up of a lot of elastic fibres, and behave like stretchable bags. There is a membrane covering the lungs called visceral pleura, and slides against another membrane that covers the inside of the chest wall, called parietal pleura. The two of these membranes essentially hold together because of surface tension, and prevent the lungs from collapsing (Bunch, 1997; Hixon, 2006; Watson, 2009).
[/toggle]
[accordion multiopen=”true”]
[toggle title=”When we expand around our waists, this is not because that area is filling with air“]
 When we inhale, the diaphragm moves downward from its dome-like shape. Its contraction causes movement of both the lower rib cage (as they are attached), and the abdomen. So, when our diaphragm flattens, it pushes the abdominal organs downwards and forwards, and creates a bulge in the epigastrium (upper abdomen).
When we inhale, the diaphragm moves downward from its dome-like shape. Its contraction causes movement of both the lower rib cage (as they are attached), and the abdomen. So, when our diaphragm flattens, it pushes the abdominal organs downwards and forwards, and creates a bulge in the epigastrium (upper abdomen).
[/toggle]
[accordion multiopen=”true”]
[toggle title=”Muscles move the ribs outward during respiration“]
 Between adjacent ribs run the intercostal muscles – there are external, internal, and an incomplete innermost layer of intercostal muscles. These muscles maintain the stability of the chest wall, and prevent it from being sucked in as the pressure falls inside the cavity during inspiration (Bunch, 1997). In other words, they keep the ribcage stable when the diaphragm contracts downwards. The main action of the external intercostals is to swing the ribs upward and outward to draw air into the lungs (Watson, 2009). When we inhale, these external muscles expand the rib cage by lifting or distancing the ribs (Cossette et al., 2010). It is then the function of the internal and innermost intercostal muscles to lower the ribs on expiration.
Between adjacent ribs run the intercostal muscles – there are external, internal, and an incomplete innermost layer of intercostal muscles. These muscles maintain the stability of the chest wall, and prevent it from being sucked in as the pressure falls inside the cavity during inspiration (Bunch, 1997). In other words, they keep the ribcage stable when the diaphragm contracts downwards. The main action of the external intercostals is to swing the ribs upward and outward to draw air into the lungs (Watson, 2009). When we inhale, these external muscles expand the rib cage by lifting or distancing the ribs (Cossette et al., 2010). It is then the function of the internal and innermost intercostal muscles to lower the ribs on expiration.
Music teachers should not only be aware of the location of the lungs and rib cage, but also have an understanding of how the various intercostal muscles function during respiration. You can read more about how air moves in and out of the lungs here.
[/toggle]
“Support the Sound!”
“The concepts of support are acknowledged to be difficult to put into words, and, for a substantial number of players, an ongoing source of mystery, confusion, and anxiety.” (Gaunt, 2004)
“Despite its importance, there is no single and unambiguous definition…the word has different shades of meaning for different singers and teachers.” (Watson, 2009)
 When a teacher says “support the sound” a student’s reaction could be any number of things when no physiological information accompanies their request. They might tense up their abdominal muscles, blow the air harder, or ‘blow from’ their diaphragms – none of which will likely have the desired effect. Teachers need to be aware of the murky waters surrounding the term ‘breath support’, and need to be aware of the physiology involved. In general terms, breath support has been described as a dynamic interaction between expiratory and inspiratory muscles (Watson, 2009). Recent scientific research can help us make sense of which muscles play a role in “supporting the sound.”
When a teacher says “support the sound” a student’s reaction could be any number of things when no physiological information accompanies their request. They might tense up their abdominal muscles, blow the air harder, or ‘blow from’ their diaphragms – none of which will likely have the desired effect. Teachers need to be aware of the murky waters surrounding the term ‘breath support’, and need to be aware of the physiology involved. In general terms, breath support has been described as a dynamic interaction between expiratory and inspiratory muscles (Watson, 2009). Recent scientific research can help us make sense of which muscles play a role in “supporting the sound.”
[accordion multiopen=”true”]
[toggle title=”Recent studies have given us working definitions of Breath Support“]
A study from the last decade on this subject began their research with a working definition that breath support was “the physiological processes used by the player to control precisely the sound production which is directly linked to the control of air flow, air velocity, and pressure required to play a specific note or musical passage” (Cossette et al., 2008). By measuring flutists playing passages both using support and not, they were able to see that inspiratory muscles (non-diaphragmatic) were being used “to keep the rib cage expanded, lung volumes higher, and the expiratory muscles relatively relaxed” (Cossette et al., 2008). This is interesting – as here we can see that the importance is more in keeping the rib cage expanded, and not in contracting the abdominal muscles – something that teachers tend to misleadingly use in their explanations.
Note that this was a study of flutists, and being a low-pressure instrument, the concept of support described here is applicable to other low-pressure instruments only – singers in particular.
[/toggle]
[accordion multiopen=”true”]
[toggle title=”Don’t forget about your neck!” state=”opened”]
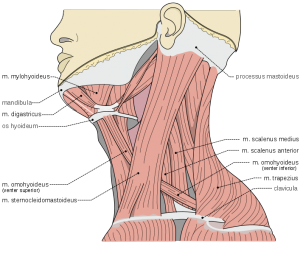 The scalene and sternocleidomastoids were more activated in the study above when the flutists were playing ‘with support’ too – these are muscles of the neck.
The scalene and sternocleidomastoids were more activated in the study above when the flutists were playing ‘with support’ too – these are muscles of the neck.
The sternocleidomastoid muscle is on the side of the neck, and runs from behind the ear forward, attaching to the top of the sternum.
The scalenus muscles (anterior, meduis, and posterior) are on the side of the neck, and their fibres run downward into the first and second ribs. Contraction of the scalenus anterior and/or scalenus medius elevates the first rib, and contraction of the scalenus posterior elevates the second rib (Hixon, 2006).
Similar activation was found in Viggo Pettersen’s muscular study of singers – he found that the activation level in these muscles was higher when the singers were told to sing in extreme registers, or maintain note for as long as possible (Pettersen, 2005).
[/toggle]
“Stand up Straight!”
 The spine consists of twenty-nine bones called vertebrae – the ribs are attached to the central section, which is made up of twelve vertebrae, the ‘thoracic vertebrae.’ The lowest vertebrae are fused together, and form part of the pelvis (Rosset & Odam, 2007).
The spine consists of twenty-nine bones called vertebrae – the ribs are attached to the central section, which is made up of twelve vertebrae, the ‘thoracic vertebrae.’ The lowest vertebrae are fused together, and form part of the pelvis (Rosset & Odam, 2007).
The vertebrae are stacked in such a way that when seen from the front, they look like a completely straight column. But, when seen from the side, we can see a series of curves. “In profile, the spine is certainly not straight; it has a cervical curve, a thoracic curve, a lumbar curve, and a sacral curve” (Nix, 2013).
To maintain anatomical alignment, especially when the awkward non-symmetrical hold of a musical instrument is thrown into the mix, teachers must be aware of the way the spine is constructed and what it attaches to. The natural curves are essential to our balance and posture. “The structure and alignment of the human skeleton is the scaffolding on which all other parts of the body depend” (Bunch, 1997).
If told to ‘stand up straight,’ a student might in fact become rigid, or might end up using more muscular effort and tension than necessary, overcompensating for their slumped body alignment. A directive that might work better could be “stand free and tall” (Nix, 2013).
[accordion multiopen=”true”]
[toggle title=”Our posture directly affects our diaphragm’s ability to move“]
When talking about breathing, we must also talk about the optimal breathing posture. The effectiveness of our diaphragm movement is very much influenced by posture. If a player or singer is slumped forward, the contents of the abdomen are forced farther upward into the thorax than when standing. The walls of the abdomen are also less free to expand, meaning that a more forceful action of the diaphragm is necessary for full inspiration. If the performer is reclined backward, the abdominal organs slump back against the spine when the diaphragm comes down on inhalation. The abdominal wall does not bulge outward, and the rib cage does not fall so far on expiration. Both of these situations result in a reduction of vital capacity – the amount of air available (Watson, 2009).
Armed with this information, teachers should be ready to educate their students on the optimal playing position for both standing and sitting scenarios; especially as many students end up in school bands, wind ensembles, or choirs, and might be sitting down rather than standing as they would in a lesson.
[/toggle]
Take a Deep Breath…
 This blog has hopefully brought to your attention some physiology relating to breathing – the diaphragm, muscles around the ribs, what ‘support’ actually means, how our posture affects our breathing, and more.
This blog has hopefully brought to your attention some physiology relating to breathing – the diaphragm, muscles around the ribs, what ‘support’ actually means, how our posture affects our breathing, and more.
All this being said, it is important to remember that there is no ONE ‘right’ way to go about breathing – it can be different for different musicians’ bodies, and of course different depending on the instrument and the musical context of a phrase.
The most important thing is that teachers and performers are able to look at physiology, and scientific studies, and apply the facts in a way that can optimize our music-making. In the case of breathing for wind players and singers, it is also important to assess statements that are passed on to us from teachers, and even printed in older method books, and ask ourselves: “is that actually how my diaphragm functions?” or “what am I actually feeling as I exhale?” Teaching will most likely still involve imagery and metaphors – for some students, their learning styles may be more suited to a combination of visual imagery (like “expand like a barrel’) and anatomical information. It is about striking the right balance for each student.
But ultimately, a deeper understanding of how our bodies function will certainly lead to improvements and optimizations of our instrumental capabilities.
[accordion multiopen=”true”]
[toggle title=”Reference List“]
Bunch, M. (1997). Dynamics of the singing voice. New York: Springer.
Cloutier, M. (2007). Respiratory physiology. Philadelphia, PA: Mosby.
Collyer, S., Kenny, D., & Archer, M. (2009). The effect of abdominal kinematic directives on respiratory behavior in female classical singing. Logopedics Phoniatrics Vocology. 34(3), 100-110. http://dx.doi.org/10.1080/14015430903008780
Cossette, I., Monaco, P., Aliverti, A., & Macklem, P. T. (2008). Chest wall dynamics and muscle recruitment during professional flute playing. Respiratory Physiology & Neurobiology, 160(2), 187-195. http://dx.doi.org/10.1016/j.resp.2007.09.009
Cossette, I., Fabre, B., Fréour, V., Montgermont, N., & Monaco, P. (2010). From breath to sound: Linking respiratory mechanics to aeroacoustic sound production in flutes. Acta Acustica United with Acustica, 96, 4, 654-667. https://doi.org/10.3813/AAA.918320
Frederick, T. (2007). The ins and outs of breathing. Canadian Musician, 29, 32.
Gaunt, H. (2004). Breathing and the oboe: Playing, teaching and learning. British Journal of Music Education, 21(3), 313-328. https://doi.org/10.1017/S0265051704005819
Hixon, T. (2006). Respiratory function in singing: A primer for singers and singing teachers. Tuscon, Arizona: Redington Brown.
Middleton, J. A. (1974). Breath function: Complement to wind instrumental musicianship. Journal of Band Research, 11(1), 3-7.
Nix, J. (2013). “You want me to do what?” twenty-first-century voice pedagogy encounters pedagogical fundamentalism. Choral Journal, 53(10), 43-51.
Pettersen, V. (2005). Muscular patterns and activation levels of auxiliary breathing muscles and thorax movement in classical singing. Logopedics Phoniatrics Vocology. 57(5-6), 255-77. https://doi.org/10.1159/000087079
Pettersen, V., & Eggebø, T. (2010). The movement of the diaphragm monitored by ultrasound imaging: Preliminary findings of diaphragm movements in classical singing. Logopedics Phoniatrics Vocology. 35(3), 105-112.
http://dx.doi.org/10.3109/14015430903313776
Rosset, L. & Odam, G. (2007). The musician’s body: A maintenance manual for peak performance. London: Guildhall School of Music & Drama.
Spillane, K. (1989). Breath support directives used by singing teachers: A delphi study. NATS Journal, 45(3), 9-57.
Thorpe, C. W., Cala, S. J., Chapman, J., & Davis, P. J. (2001). Patterns of breath support in projection of the singing voice. Journal of Voice: Official Journal of the Voice Foundation, 15(1), 86-104. http://dx.doi.org/10.1016/S0892-1997(01)00009-1
Watson, A. (2009). The biology of musical performance and performance-related injury. USA: Scarecrow Press.
Watson, P., & Hixon, T. (1985). Respiratory kinematics in classical opera singers. Journal of Speech, Language, and Hearing Research. 28, 104-122. http://dx.doi.org/10.1044/jshr.2801.104
[/toggle]
[accordion multiopen=”true”]
[toggle title=”Image List“]
Barbara Hannigan, soprano, Reinbert de Leeuw, piano, Lelli e Masotti, via Wikimedia Commons
https://commons.wikimedia.org/wiki/File:Barbara_Hannigan.jpg
{kind=link}
Diafragma ademhaling, via Wikimedia Commons
https://commons.wikimedia.org/wiki/Category:Respiration#/media/File:Diafragma_ademhaling.gif
{kind=link}
Dorsal Ventral Body Cavities, via Wikimedia Commons
https://commons.wikimedia.org/wiki/File:Dorsal_Ventral_Body_Cavities.jpg
{kind=link}
Trunk Muscles, via Wikimedia Commons
https://commons.wikimedia.org/wiki/File:Illu_trunk_muscles.jpg
{kind=link}
Wine barrels at the storage room at Tonelería Nacional, Chile, Gerard Prins, via Wikimedia Commons
https://commons.wikimedia.org/wiki/File:Oak-wine-barrel-at-toneleria-nacional-chile.jpg
{kind=link}
The Lung Pleura, via Wikimedia Commons
https://commons.wikimedia.org/wiki/File:2313_The_Lung_Pleurea.jpg
{kind=link}
Intercostal Muscles Animation Gif, via Wikimedia Commons.
https://commons.wikimedia.org/wiki/File:Internal_intercostal_muscles_animation.gif
{kind=link}
Flute by Lifesupercharge, Flickr.com, via Creative Commons CC BY-NC-SA 2.0
https://c1.staticflickr.com/6/5043/5377303476_3ee0932cc8_b.jpg
{kind=link}
Musculi coli base, Olek Remesz, via Wikimedia Commons
https://commons.wikimedia.org/wiki/File:Musculi_coli_base.svg
{kind=link}
La voûte formée par le muscle diaphragm, via Wikimedia Commons
https://commons.wikimedia.org/wiki/File:La_vo%C3%BBte_form%C3%A9e_par_le_muscle_diaphragme.gif
{kind=link}
Opera singer by Alfred Schmidt, via Wikimedia Commons
https://commons.wikimedia.org/wiki/File:Opera_singer_by_Alfred_Schmidt.jpg
{kind=link}
[/toggle]
Leave a Reply