
When you play your wind instrument, does air ever leak out your nose?
Any musician who plays a wind instrument is probably familiar with embouchure fatigue, or leaking around the embouchure. Occasionally, however, other parts of the breathing apparatus fatigue, or don’t function as well as they should. One major dysfunction is called Velopharyngeal Insufficiency (VPI) a potentially career-altering or career-ending condition. This occurs when the velum – also known as the soft palate – fails to close up properly against the back of the throat. This allows air to escape through the nose while playing, or singing, instead of being directed through the instrument or mouth. Evans and colleagues noted that the prevalence among student musicians is as high as 39%.
What does it sound/feel like?
When playing a wind instrument, the musician will feel and/or hear a “snort” or “hiss” of air, rustling up through the nose. In some cases, only the musician notices it, in other cases it is also readily audible to those nearby.
How should the soft palate function?
Here is an example of a horn player viewed from the side. In this case, she is NOT experiencing VPI, but from the video, one can see the soft palate lift to touch the back of the throat, as it should.
What happens during VPI?
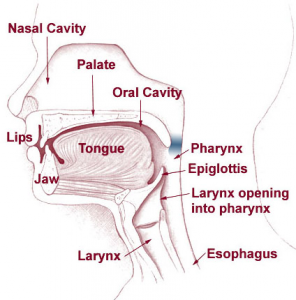
Here is a diagram that shows the basic structure of the upper respiratory tract. The area marked in blue is the general area of the throat where Velopharyngeal Insufficiency occurs. In musicians experiencing VPI the “flap” of muscle (which in the diagram is in a resting position, directly to the left of the blue area) fails to lift up correctly, compared to what can be seen in the video.
(Image Source: Creative Commons)
Who is at risk?
Any wind instrument player, or even singer, can be affected by this condition. The higher risk occurs when one plays an instrument with a higher intra-oral pressure: the pressure that builds up inside the mouth and throat when playing a note. Here is a chart of some instruments and their intra-oral pressures measured in millimeters of mercury (mmHg): (What is mmHg?)
Highest Pressures on Different Instruments Played Fortissimo
| Instrument | Intra-oral Pressure (mmHg) |
| Trombone | 126 |
| C-Trumpet | 125.8 |
| French Horn | 115.9 |
| Bassoon | 89.7 |
| Clarinet | 86.4 |
| Oboe | 80.8 |
| Flute | 77.8 |
| Tuba | 77.6 |
| Piccolo | 58.3 |
| Alto Saxophone | 56.2 |
| English Horn | 54.7 |
| Alto Recorder | 11.6 |
Chart information obtained from: Videoendoscopic Diagnosis and Correction of Velopharyngeal Stress Incompetence in a Bassoonist (Gordon et. al, 1994). They also found that the pressure required for normal speech rarely exceeds 6 mm/Hg.
It’s important to note the pressure required for instrumental play is much higher than for regular speech, and this therefore places much more demand on the velopharyngeal muscles than normal. (Additional information on pressures in this article by Bennett and Hoit.)
What causes VPI?
If this happens, am I doing something wrong?
The answer here is…maybe! As with many disorders affecting musicians, there is seldom one isolated cause. It is important to distinguish between factors that a musician can and cannot control.
It’s possible that you have an underlying neurological condition, or structural defect of the soft palate. Thorough evaluation by an Otolaryngologist is required to determine this. The musician suffering from this condition should play his or her instrument while the doctors perform a nasoendoscopy. (Please refer to this article for a more detailed description of the purpose of a nasoendoscopy (McVicar et al., 2002)). They will insert a flexible camera into the nose to observe the functioning of the soft palate. This will help the doctor to determine if there is anything structurally problematic, or if it is not functioning correctly with regular speech. That being said, it is important that one play one’s instrument for the doctor because, as noted above, the pressures required for speech and instrumental play are much different!
Factors under the musician’s control
The five following are the most common causes of VPI that are essentially under the musician’s control. (Trollinger et al., 2017)
1. Muscular fatigue (of the palate muscles themselves): This will differ for each individual. As with any muscle in the human body, there is a physiological limit to the amount of stress/strain a muscle can sustain before it will no longer function correctly.
2. Performance-related stress: nervousness, anxiety about performing, etc.
3. Other kinds of stress: school, work, other life events
4. Prolonged periods of intense music-making: long rehearsals, long coachings, many performances in a row
5. Returning to practice after a significant time away: weeks, months, or years away from the instrument, followed by a rapid return to practice/play intensity adhered to before the break occurred.
While certain kinds of stresses are unavoidable, musicians should strive to adopt practice and performance strategies that minimize the “self-inflicted” risks of developing VPI. Christine Guptill and Christine Zaza (2010) describe practice strategies in their article that focus more generally on musculoskeletal injury prevention, but as the #1 cause of VPI is muscular fatigue, their suggestions can easily apply to any music student, performer, or teachers.
Practice Strategies
(Source: Guptill and Zaza, 2010)
Warm-up
~ In addition to the usual musical warmup of scales, long tones, and patterns, musicians should also do a general physical warm-up.
~Deep breathing exercises.
~ Emphasize easy playing that demands little technical requirements.
Breaks
Incorporate several kinds of breaks:
~Microbreaks
~Breaks away from playing
~Full breaks
Microbreaks consist of breaks of around thirty seconds, or even counting through the rests in a piece of music instead of jumping directly to the next part. Guptill mentions that “for wind instrumentalists, counting rests can greatly increase perceived stamina for a long recital and may not only prevent injury, but may also improve students’ self-confidence.”
Breaks away from playing involve doing something different to the normal requirements of playing. This could involve changing position (standing vs. seated) while simply reading through the music, or even marking the part, or listening to a recording. It should not involve using the muscles that are normally used for play (e.g. fingering through parts, practicing tonguing)
Of course, full breaks away from the practice room where the musician completely forgets about practicing are also beneficial. The length of such a break can be determined by the musician, depending on practice habits, or work/study circumstances. In Guptill and Zaza’s article, they note that no specific length of break can be determined as the most effective. The instrument the musician plays, his or her current skill level, and also familiarity with the piece being played all affect the length of break required.
Posture and playing position
Adopting a healthy, aligned posture while playing can help contribute to decreased tension throughout the body, including the throat, face, and embouchure. It is unclear if a “tense” style of playing directly contributes to VPI, but it is wise nonetheless to remain comfortable while playing.
Technique
The student should develop the technique required to play repertoire with ease . Having patterns and scales and long tones well established allows the student to learn music in less time and with fewer repetitions
Repetition
Repetition is important to learning material, but can also be a risk factor for injuries. In the case of VPI, this would mean overusing or taxing the soft palate muscles.
It is important to use smart practicing techniques to avoid overtaxing muscles, regardless of instrument, such as:
~Practicing short chunks of music, rather than continually “running it from the top.”
~Figure out what is truly not working in your performance of the music and focus on that.
~Practice at whatever tempo allows you to remain relaxed – increase tempo afterwards.
~Mental practice: thinking about the music, and studying it away from the instrument helps reduce the number of repetitions that may be needed to learn it.
Pacing
~Distribute practice sessions over time. Avoid “cramming” practice sessions before important performances or lessons.
~If an increase in total practice time is needed, allow enough time to do it gradually.
What can be done medically to resolve the issue?
Speech Therapy
As a conservative approach, speech therapy may be undertaken. Often, if there is some underlying speech impediment that may be affecting the soft palate, it can be discovered here. If this is the case, clinicians treating VPI will recommend at least a few months of speech therapy before any other procedures are considered.
Augmentation
This involves injecting a substance (Teflon has been used, and occasionally the patient’s abdominal fat) into the soft palate to bulk it up, in order to improve closure of the soft palate against the throat. A video of an oboist undergoing this procedure can be seen here:
Surgery
As a last resort, various surgeries can be performed to correct the issue. The exact type of surgery depends on which of the velopharyngeal muscles are contributing to the lack of closure.
One type of surgery that appeared to have fewer complications was performed on an 18-year-old clarinet player. McVicar and colleagues performed a Sphincter Pharyngoplasty and state that the procedure was simpler as it is done in one stage, and the velum (soft palate) does not need to be violated in order to do the surgery.
Keep the communication lines open!!
Students often hold their instrumental teachers in very high esteem, as the teacher is providing the student with such valuable expertise. When it comes to matters of physical impairment, however, the instrumental teacher, though well-meaning, might not know enough! In their article addressing VPI, authors Evans, Ackerman, and Driscoll mention in their abstract that this lack of knowledge can actually contribute to insufficient advice from most teachers to their students. This often leads students to ignore early warning signs and subsequently endure much longer recovery times. That being said, keeping an open communication between student, teacher, and clinician should be encouraged. That way, awareness of the condition, and dissemination of this knowledge, will be improved.
[toggle title=”References”]
Bennett, K., & Hoit, J. D. (January 01, 2013). Stress velopharyngeal incompetence in collegiate trombone players. The Cleft Palate-Craniofacial Journal : Official Publication of the American Cleft Palate-Craniofacial Association, 50, 4, 388-93. DOI: https://doi.org/10.1597/11-181
Conley, S. F., Beecher, R. B., & Marks, S. (1995). Stress velopharyngeal incompetence in an adolescent trumpet player. Annals of Otology, Rhinology & Laryngology, 104(9), 715-717. DOI: https://doi.org/10.1177/000348949510400909
Evans, A., & Ackermann, B. (2013). How to identify and manage stress VPI: Recommendations for wind instrumental teachers and students. In Proc. Int. Symp. Perform. Sci. (Vol. 2013, pp. 657-662).
Source: http://www.performancescience.org/ISPS2013/Proceedings/Rows/148Paper_Evans.pdf
Evans, A., Ackermann, B., & Driscoll, T. (January 01, 2010). Functional anatomy of the soft palate applied to wind playing. Medical Problems of Performing Artists, 25, 4, 183-9. http://mcgill.worldcat.org/oclc/704810453
Evans, A., Driscoll, T., & Ackermann, B. (October 01, 2014). A Delphi survey on diagnosis and management of stress velopharyngeal insufficiency in wind musicians. International Journal of Speech-Language Pathology, 16, 5, 445-455.
Gordon, N. A., Astrachan, D., & Yanagisawa, E. (1994). Videoendoscopic diagnosis and correction of velopharyngeal stress incompetence in a bassoonist. Annals of Otology, Rhinology & Laryngology, 103(8), 595-600. DOI: https://doi.org/10.1177/000348949410300803
Gray, H., Williams, P. L., & Bannister, L. H. (1995). Gray’s anatomy: The anatomical basis of medicine and surgery. New York: Churchill Livingstone.
Guptill, C., & Zaza, C. (January 01, 2010). Injury prevention: what music teachers can do. Music Educators Journal, 96, 4, 28-34. DOI: https://doi-org.proxy3.library.mcgill.ca/10.1177/0027432110370736
Guptill, C. (January 01, 2011). The lived experience of working as a musician with an injury. Work (reading, Mass.), 40, 3, 269-80. DOI: https://doi.org/10.3233/WOR-2011-1230
McVicar, R., Edmonds, J., & Kearns, D. (2002). Sphincter pharyngoplasty for correction of stress velopharyngeal insufficiency. Otolaryngology–Head and Neck Surgery, 127(3), 248-250. DOI: https://doi.org/10.1067/mhn.2002.127382
Trollinger, V. L., & Sataloff, R. T. (2017) Respiratory Behaviors and Vocal Tract Issues in Wind Instrumentalists. Professional Voice: Science and Art of Clinical Care, 4, Ch. 63.
[/toggle]
Leave a Reply