
Young musicians are often told that the more they practice, the better they will become. Therefore, they dedicate themselves in the practice room every day to try to refine their technique. To achieve perfection, or close to it, musicians sometimes must repeat awkward motions with their hands which can lead to tension build-up and eventually injury.
How often do Musicians get injured?
In 2012, a survey done in Australia, which included eight major orchestras, found that 84 percent of the musicians had experienced pain or injuries that prevented them from playing at maximum capacity.
Fifty percent of the participants were still dealing with pain at the time of the survey.
Twenty-eight percent had to take at least one day off because of pain.
Less than fifty percent of the musicians have reported being injured fully recovered.
Don’t be afraid when you get injured, you are not alone!
- Gary Graffman– Famous piano soloist who hid his injury until it was too late, thus, his right hand is permanently injured
- Leon Fleisher– Lost the use of his right hand, due to Focal Dystonia
- David Leisner – World renown guitarist also with Focal Dystonia
- Peter Oundjian- first violinist of the Tokyo string quartet resigned due to left hand tendonitis
Risk Factors
Musicians are especially prone to work related musculoskeletal disorders (WMSDs), such as carpal tunnel syndrome, t endonitis and thoracic outlet syndrome. WMSDs can be caused by hand movements such as bending, straightening, gripping, holding, twisting, clenching and reaching. Although these activities are harmless in normal activities, but when these motions are repeated many times and with unnatural force, it can be problematic. Musicians often must stay seated in a constrained position during orchestra rehearsals, repeat difficult hand motions and play for long periods of time. These are work patterns that can lead to WMSDs.
endonitis and thoracic outlet syndrome. WMSDs can be caused by hand movements such as bending, straightening, gripping, holding, twisting, clenching and reaching. Although these activities are harmless in normal activities, but when these motions are repeated many times and with unnatural force, it can be problematic. Musicians often must stay seated in a constrained position during orchestra rehearsals, repeat difficult hand motions and play for long periods of time. These are work patterns that can lead to WMSDs.
(Canadian Centre for Occupational Health & Safety, 2014)
[toggle title=”Tendonitis”]
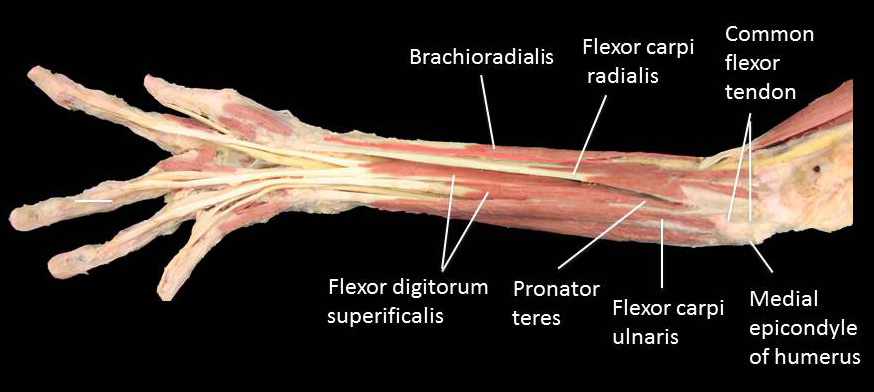
To fully understand what tendonitis is, besides my arm hurts, we must look at the anatomy of one’s arm first. Tendons are the tissues that connect muscles and bones. They are very strong, and 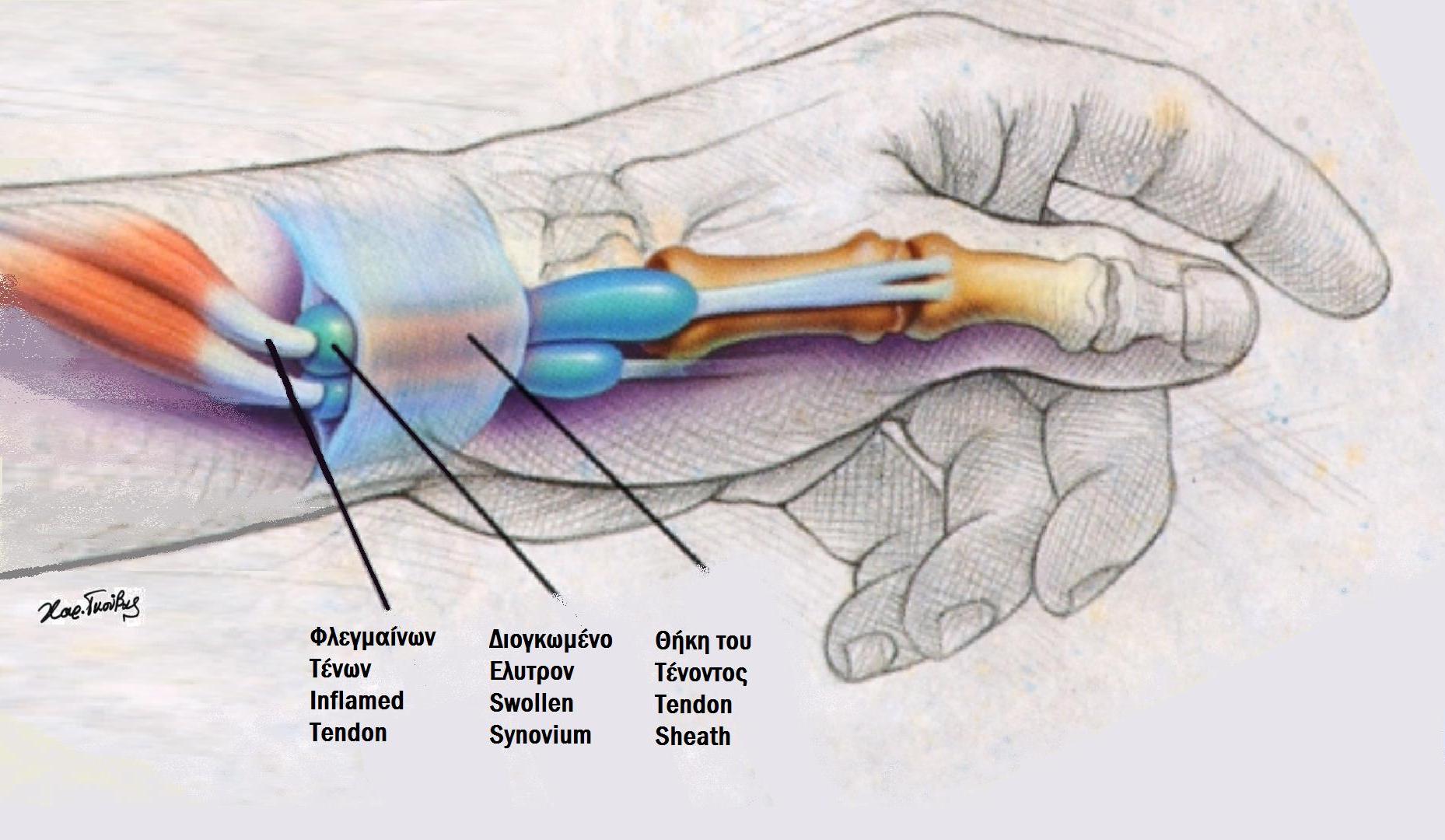 have one of the highest tensile strengths among soft tissues. Although strong, tendons still get restricted by the way we move our wrists. Tendon sheaths are what allow tendons to move freely and smoothly. There are two layers of synovial membranes, which form a double cylinder with an inner layer warped directly around the tendon itself. The thin film of synovial fluid between the two layers ensures that the tendon can slide smoothly into the sheaths. When our wrists are held in awkward positions for too long, the friction between our tendons and the sheaths can get damaged. Tendonitis located at the elbow area is called epicondylitis or “tennis elbow”. It is the most common type of tendonitis in musicians, especially string players. It may occur when tendons become inflamed due to forceful repetitions of rotating the hand and wrist when there is too much friction between tendons and their tendon sheaths, irritation and damage can happen due to inflammation and swelling. Signs of tendonitis usually include pain in the wrist and a “burning” feeling (Watson 2009).
have one of the highest tensile strengths among soft tissues. Although strong, tendons still get restricted by the way we move our wrists. Tendon sheaths are what allow tendons to move freely and smoothly. There are two layers of synovial membranes, which form a double cylinder with an inner layer warped directly around the tendon itself. The thin film of synovial fluid between the two layers ensures that the tendon can slide smoothly into the sheaths. When our wrists are held in awkward positions for too long, the friction between our tendons and the sheaths can get damaged. Tendonitis located at the elbow area is called epicondylitis or “tennis elbow”. It is the most common type of tendonitis in musicians, especially string players. It may occur when tendons become inflamed due to forceful repetitions of rotating the hand and wrist when there is too much friction between tendons and their tendon sheaths, irritation and damage can happen due to inflammation and swelling. Signs of tendonitis usually include pain in the wrist and a “burning” feeling (Watson 2009).
[/toggle]
[toggle title=” Carpal Tunnel Syndrome”]Carpal tunnel syndrome (CTS) is the most common type of nerve entrapment in the arm from which musicians suffer from. The problem usually occurs on the median nerve territory of the hand, which runs from the forearm into the palm of the hand and becomes compressed at the wrist. The median nerve controls the thumb and the first three fingers, therefore CTS can cause numbness, burning and itching feeling of the palm and the fingers. Symptoms usually occurs at night because people often sleep with flexed wrists. (National institute of Neurological Disorders and Stroke 2017)
Musicians are prone to have inflamed flexor tendons because they often keep their hand in a constant flexed position, or constantly changing from
extension to flexion. Flexor tendons are surrounded by a synovial sheath, which passes through the flexor retinaculum. When the tendon is swollen, and
inflamed, it overproduces synovium, which is a lubricant that allow tendons to move smoothly within the sheath. When synovium is overproduced, it turns into a sticky compound, which increases the friction between the tendon and the sheath, that may ultimately leads to more inflammation and develop into a problem called tenosynovitis. If the condition is left untreated it can lead to “trigger finger”, which is when fingers or thumb become locked . (Jameson, 1998)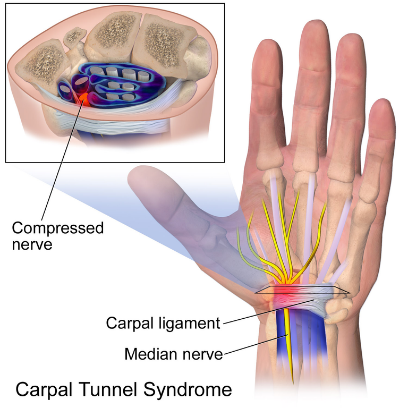
Non-surgical Treatments
Wrist Splinting- By holding the wrist in one position with a splint during sleep can relieve symptoms like tingling and numbness.
Corticosteroids- Doctor might inject corticosteroids, sometimes with the guidance with ultra sound, into the carpal tunnel to relieve pain. It will decrease the swelling and inflammation therefore lessen the pressure on the median nerve.
Acupuncture- Needles and low-level lasers are used to stimulate acupuncture points on the affected hand.
(Carlson, 2010)
Surgical treatment
Surgical treatments are usually considered when nonsurgical treatments have failed or the affected hand is too severe. The surgery is very safe, and the goal is to relieve pressure on the median nerve at the wrist. A small cut will be made over the palmar side of the wrist and then release the ligament that covers the carpal tunnel. Once the ligament is released, the carpal tunnel will increase in size and the pressure is relieved. Dressing is placed over the surgical wound after the surgery, most people feel comfortable with ordinary activities right after and can return to light jobs in three weeks. (William, 2016)
[/toggle]
[toggle title=”Quervain’s Syndrome”]The syndrome was named after the surgeon, Fritz de Quervain, who first identified it in 1895. He published five case reports where patients had tender, thickened first dorsal compartment at the wrist. The syndrome is caused by the inflammation of tendons, specifically the extensor polices brevis and the abductor polices longs. 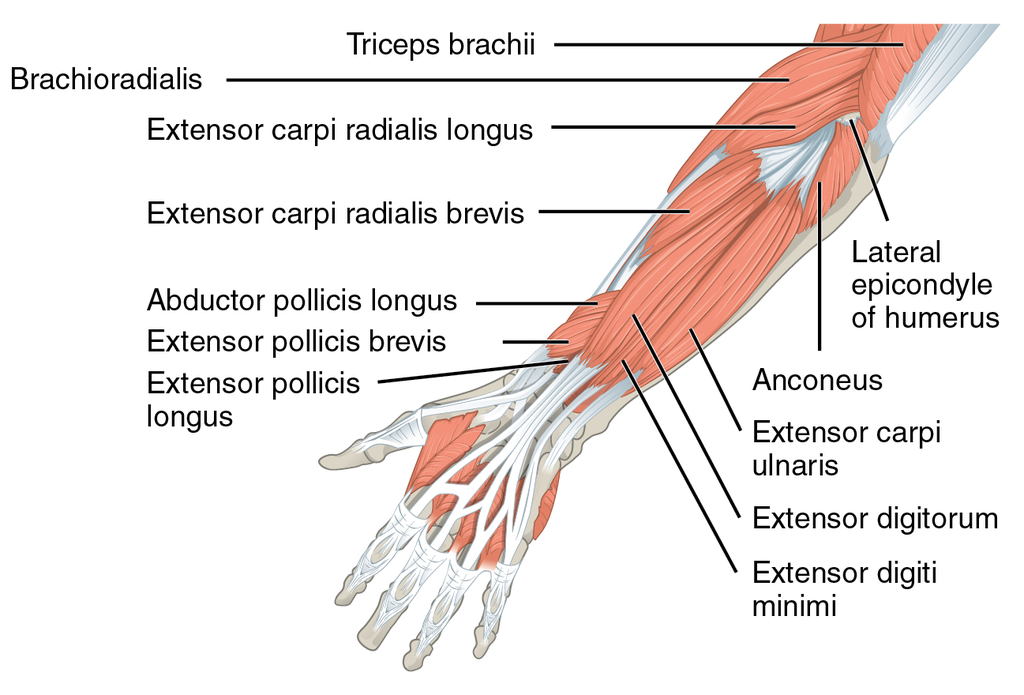
These two tendons are located at the side of the wrist. Since the two tendons are secured so tightly against the radial styloid by the overlying extensor retinaculum, any enlargement of it will limit the tendon’s ability to glide through the tendon sheaths. However, for musicians, it is more likely to 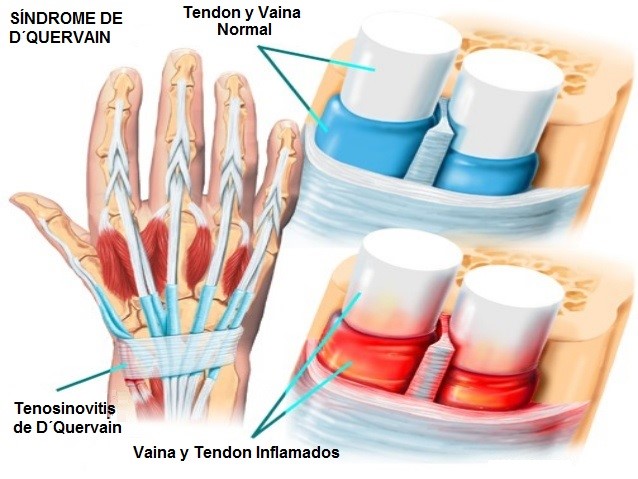 happen because of repetitive motions every day on their instruments and demanding performance schedules. (Medscape, 2016)
happen because of repetitive motions every day on their instruments and demanding performance schedules. (Medscape, 2016)
Symptoms can include pain on the thumb side of the wrist, and is especially enhanced while lifting the thumb. Due to the swollen sheaths, tendons might make a squeaking sound when trying to move within. It is possible that fluid-filled cyst may bulge through the skin at the affected area. (American Academy of Family Physicians, 2014)
Examination
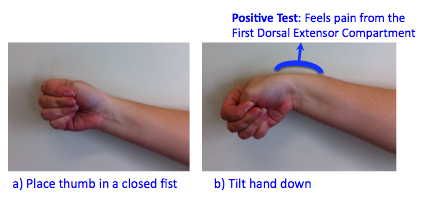
To determine if someone has quervain’s syndrome or not, the patient will be asked to perform a Finkelstein test. The patient will place his thumb against the hand, and then making a fist with the fingers crossed over the thumb, then bending the wrist towards the little finger (diagram below). It will be very painful if the patient has quervain. (American of Orthopedic Surgeons, 2013)
Non-surgical treatments:
Some initial treatments include applying ice on the affected area to reduce swelling, keeping the thumb and wrist straight with a splint and brace, and injecting corticosteroids. (American Academy of Family Physicians, 2014)
Surgery
Surgery will require local or regional anesthesia; the goal is to create more room for the tendons. Surgeon will perform a 3-cm incision over the prominent thickening of the first dorsal compartment. When there is more space, tendons will stop rubbing against each other and therefore reduce the inflammation. Even though the surgery is a simple, complications can occur and could be permanent. (Medscape, 2016)[/toggle]
[toggle title=”Prevention”]Injuries are much easier to prevent than to treat. A few examples of ways to help prevent an injury.
Overuse– It is important to take breaks during a practice session because there is a limit to how long tendons and muscles can work before needing to rest. By consistently playing non-stop will overwork the human body and lead to problems. Even if a musician has good technique and plays with ease, the fluid that keeps tendons slide smoothly into their sheaths will become depleted if playing during a long period without rest. Therefore it is important to stop before friction between tendons start to occur. (Klickstein, 2012)
Warm-up– It is a process that musicians don’t do seriously enough. Sometimes they get off their car and dive right into their demanding three hour rehearsals. Warming up before a concert, practice sessions, rehearsal is important because it increases blood flow in the muscles that we use to play our instruments and increases lubrication in our joints. It is important not to try playing everything at max tempo from the start. (Klickstein, 2012)
Smart practicing is probably the most important thing to keep in mind for any musician because ultimately it will pay off in a career longevity and better music making. [/toggle]
[toggle title=”References”]
References
Ackermann, B. (2012). Muscuoskeletal pain and injury in professional orchestral musicians in Australia. Medical Problems of Performing Artists, 27(4) 181-187 Link: https://www.ncbi.nlm.nih.gov/pubmed/23247873
Brandfonbrener, A. (2003). Musculoskeletal problems of instrumental musicians. Hand Clinic, 19, 231-239 Link: https://doi.org/10.1016/S0749-0712(02)00100-2
Carlson, H. (2010). Current options for nonsurgical management of carpal tunnel syndrome. International journal of clinical rheumatology, 5(1) 129-142. Link: https://doi.org/10.2217/ijr.09.63
Carpal Tunnel Syndrome Causes, Symptoms, Treatment – Carpal Tunnel Syndrome Surgery. (n.d.). Retrieved April 15, 2017, from http://www.emedicinehealth.com/carpal_tunnel_syndrome/page4_em.htm#carpal_tunnel_syndrome_surgery
Crabb, D. (1980). Hand injuries in professional musicians. The Hand, 12(2) 200-208
De Quervain Tenosynovitis Treatment & Management. (2016, August 24). Retrieved April 15, 2017, from http://emedicine.medscape.com/article/1243387-treatment#d14
Jameson, T. J. (1998). Repetitive strain injuries: the complete guide to alternative treatments and prevention. New Canaan, Conn: Keats Publishing.
Klickstein, Gerald. (2009). The Musician’s Way: A Guide to Practice, Performance, and wellness. US: Oxford University press.
Lee, H. (2013). Musicians’ Medicine: Musculoskeletal problems in string players. Clinics in Orthopedic Surgery, 5(3) 155–160 Link: https://doi.org/10.4055/cios.2013.5.3.155
Oestreich, J. R. (1996, August 26). In Music as Well as Sports, Injuries Can End a Career. Retrieved April 15, 2017, from http://www.nytimes.com/1996/08/27/arts/in-music-as-well-as-sports-injuries-can-end-a-career.html
Rettig, A. (2001). Wrist and Hand Overuse Syndromes. Clinics in Sports Medicine, 20(3) 591-611 Link: http://dx.doi.org/10.1016/S0278-5919(05)70271-4
Uhl, T. Rehabilitation Concepts and supportive Devices for Overuse injuries of the upper extremities. Clinics in Sports Medicine, 20(3) 621-639 Link: http://doi.org/10.1016/S0278-5919(05)70273-8
Winspur, I. (2003). Controversies surrounding “misuse,” “overuse,” and “repetition” in musicians. Hand Clinics, 19(2) 325-329 Link: http://dx.doi.org/10.1016/S0749-0712(02)00124-5
Watson, AHD. (2009). The biology of musical performance and performance-related injury. UK: Scarecrow Press.
[/toggle]
[toggle title=”Image references”]
MITO orchestra sinfonica. via https://commons.wikimedia.org/wiki/File:MITO_Orchestra_Sinfonica_RAI.jpg
{kind=link}
Common flexor tendon. via https://commons.wikimedia.org/wiki/File:Common_flexor_tendon3.jpg
{kind=link}
Carpal tunnel syndrome. via https://commons.wikimedia.org/wiki/File:Carpal_Tunnel_Syndrome.png
{kind=link}
120 Muscles that move the forearm antebrach. via https://commons.wikimedia.org/wiki/File:1120_Muscles_that_Move_the_Forearm_Antebrach._Sup._Ext._Sin.png
{kind=link}
Quervain’s syndrome. via https://upload.wikimedia.org/wikipedia/commons/6/6b/Sindrome-de-quervain.jpg
{kind=link}
Finkelstein test. via https://commons.wikimedia.org/wiki/File:Finkelstein%27s_test2.png
{kind=link}
[/toggle]