
Difficulty is an unavoidable aspect in our lives as musicians, each challenge gives us the opportunity to grow and learn. On our better days, the practice sounds good and the difficulties feel effortless; on our bad days, it seems like we’ve never touched our instrument ever before. It’s no mystery that getting better at our instruments requires a great deal of time, effort, grit, and commitment. For some of us, the standard we measure ourselves to grows higher and higher as we become more and more proficient. We all have our reasons to push ourselves: to win that audition, to qualify for this competition, to impress our colleagues and mentors – all common reasons that stoke the fires of motivation.
That fire can sometimes drive us to overextend ourselves. Usually, our first instinct is to push our minds and bodies for more and harder practice; but doing so at an unsustainable pace and duration can lead us to problems of pain in the short term, injury in the medium term, and musculoskeletal disorders in the long term. If you’re reading this, you’re likely a music student in a university or conservatory; and thus pretty aware of the pervasiveness of pain and injuries in musicians. If you aren’t aware, then: Yes! Professional musicians by and large, are not exactly the most healthy bunch. Some are dealing with pain while they play, some have had to set aside playing to recover from injuries accrued over their career, while some may never play again from developing chronic or degenerative conditions like focal dystonia or severe tendonitis.
This blog seeks answers to how musicianship affects pain and pain processing in musicians by looking at scientific research to provide musicians with a more informed understanding of our pain awareness. We’ll look at several scientific studies exploring links between physical pain and musicians. Does being a musician affect our experience of pain? Are musicians more sensitive and risk-averse to pain because they are obligated to maintain a level of physical wellbeing to play well? Or, are musicians more resistant and resilient to pain because t acknowledged that pain is a byproduct of overcoming difficulties?
We’ll start with the physiology of pain, explore some research investigating this very problem, and arrive at conclusions that will hopefully help make informed choices in pain and risk assessment.
Physiological Components of Pain
Pain Receptors and Primary Afferents:
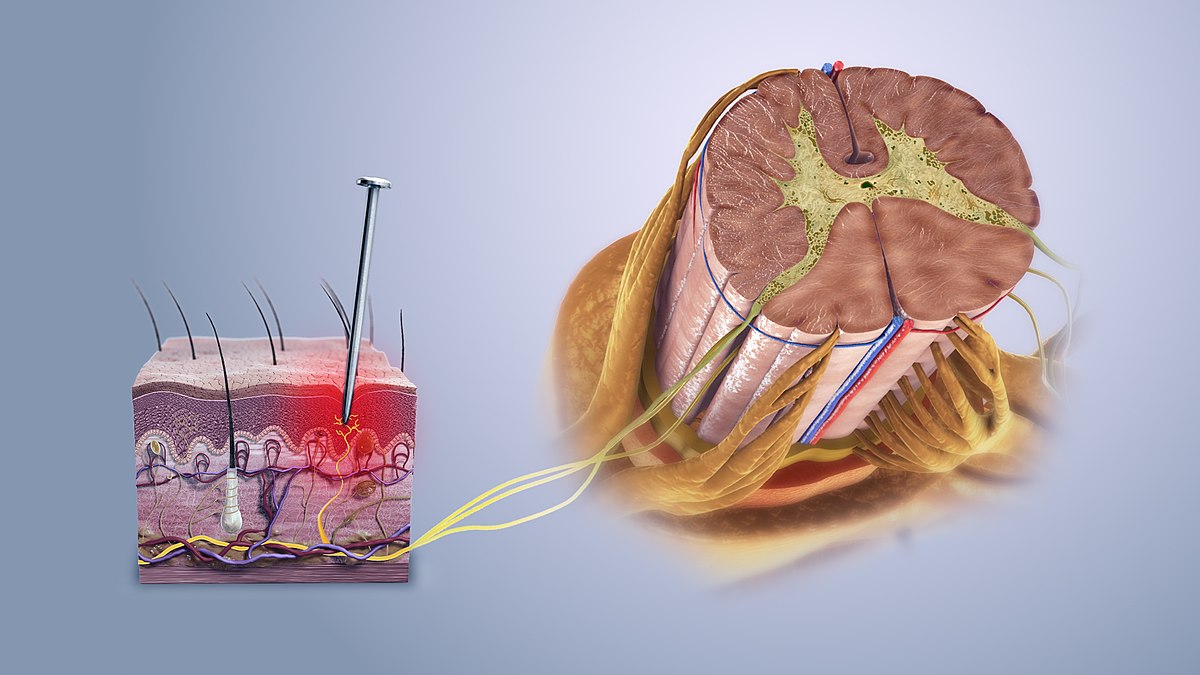
Nociceptors are specialized nerve receptors tasked with detecting harmful stimuli. When potentially damaging events occur, these receptors convert the harmful stimuli into electrical signals. This information is then transmitted to the central nervous system via two types of nerve fibers. Aδ(A delta) fibers quickly carry signals responsible for the sharp, well-localized pain you feel when you experience a quick, pricking sensation. In contrast, C fibers relay information more slowly, resulting in a dull, aching, and long-lasting pain (Steeds 2013).
Central Nervous System Processing and Dorsal Horn Processing
Once the pain signals are generated, they travel along Aδ and C fibers to the dorsal horn (rearward aspect) of the spinal cord, where the initial processing begins. In this area, various types of neurons including: nociceptive-specific, wide dynamic range, and low-threshold neurons interact in complex ways through excitatory and inhibitory signals. This interplay serves to contextualize the signal with other sensory neurons and prioritize more important pain information before it ascends to higher brain centers (Steeds, 2013).
Ascending Pathways
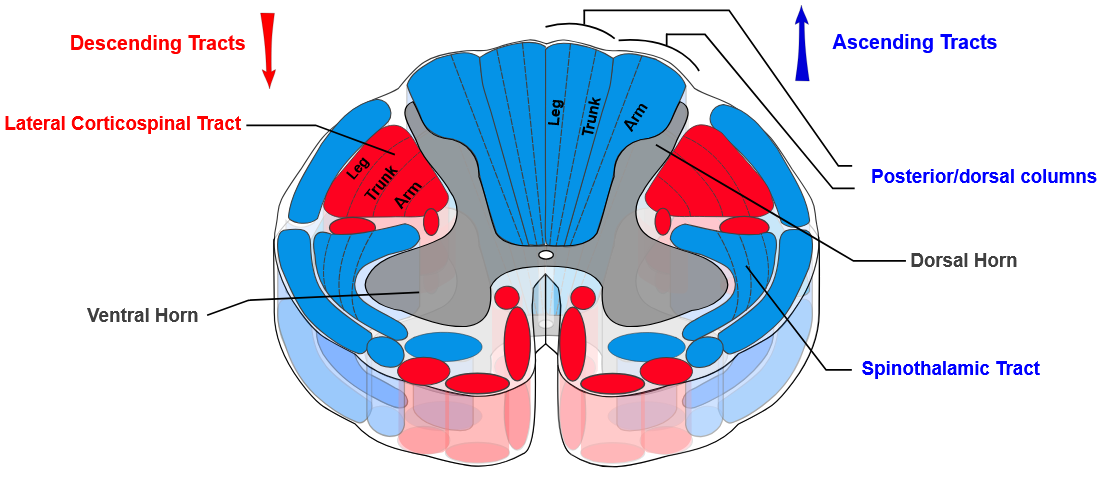
After processing in the dorsal horn, pain signals are relayed upward to the brain through ascending pathways. Specifically, the spinothalamic and spinoreticular tracts (see figure 1) convey both fast, sharp pain and slow, dull pain to the thalamus and other relevant brain regions. Once these signals reach the brain, they are further interpreted and felt to enable us to respond to the underlying cause of pain (Steeds, 2013).
Descending Pathways
Not only does the brain receive pain signals, but it also actively participates in moderating them through descending pathways. Regions in the midbrain and medulla send inhibitory neurotransmitters (i.e., serotonin, endorphins, and norepinephrine) back down to the spinal cord. These chemicals help block or lessen pain transmission, acting as an internal control system to moderate and reduce the intensity of pain (Steeds, 2013).
Forays into the Research
In this section, we’ll look at six studies investigating how musicians process and respond to pain. I’ll present their aims and methods, and their findings. Each of these studies are worth highlighting by themselves since each requires some careful reading. In my perusing of the literature, my early and confusing conclusions were that being a musician made an individual both sensitive and insensitive to pain Some nuances are necessary in understanding these, and context is needed to appreciate these studies. To keep track of the potentially confusing conclusions, I’ll ask the help of some friends to keep a running tally after each study: did they find musicians less, more, or comparable to non-musicians?

Frogs are cold-blooded animals that, unlike us mammals, are able to adapt their body temperature to their environment to maintain equilibrium. If you put the frog in room-temperature water and slowly heat it up, the frog won’t realize what’s happening. It just keeps adjusting to the temperature until it’s too hot. Once they’ve expended too much of their energy tolerating and adjusting to the rising heat, they’re unable to jump out. This illustrates a metaphor for how people can gradually acclimate or ignore to discomfort, pain, or minor issues until they accumulate into serious and potentially irreversible problems.
Exercise- and stress-induced hypoalgesia in musicians with and without shoulder pain: A randomized controlled crossover study (Kuppens. et al, 2016)
This study set out to explore how both physical and emotional stress influence pain sensitivity. The researchers recruited participants into two groups: healthy musicians and musicians with shoulder pain. They measured participants’ pressure pain thresholds (a self-report method) before and after exposing them to two distinct stressors—a strenuous isometric shoulder exercise and an emotionally stressful task.
The findings revealed that both physical exertion and emotional stress were associated with a reduction in pain sensitivity. Stress-induced hypoalgesia is the body’s tendency to reduce its perception of pain when it’s under acute stress. It is one aspect of our sympathetic nervous response (fight or flight) of our autonomic nervous system. Importantly, the study noted that a comparison of their results to norms between healthy and pained individuals, there were no significant differences between musicians and non-musicians populations. In other words, the stress-induced reduction in pain perception appeared to operate similarly regardless of an individual’s musical background or the presence of shoulder pain.
Analysis of deep tissue hypersensitivity to pressure pain in professional pianists with insidious mechanical neck pain (Linari-Melfi et al, 2011)
This study set out to explore how neck pain in musicians might affect overall pain sensitivity. Researchers recruited two groups of professional pianists with and without neck pain. They measured pressure pain thresholds across several key areas of the body: neck, shoulder, second metacarpal, and tibialis anterior.
Interestingly, pianists with neck pain exhibited increased sensitivity in distant, non-symptomatic areas such as the hands and legs. However, when tested for pressure pain in the neck, the area of injury, pain ratings between injured and healthy pianists were not significantly different. This finding suggests that localized neck pain in musicians might be linked with a broader systemic sensitization, a phenomenon that could have implications for both diagnosis and treatment strategies in managing musculoskeletal pain.
Impact of chronic pain on use-dependent plasticity: Corticomotor excitability and motor representation in musicians with and without pain (Zamorano et al, 2024)
This study delved into how chronic pain might influence the adaptive changes that result from long-term musical training. Researchers compared three groups: pain-free non-musicians, musicians suffering from chronic upper limb or neck pain, and pain-free musicians. Using transcranial magnetic stimulation (see figure 2), they measured key parameters of the first dorsal interosseous muscle (the meaty muscle connecting your thumb to the rest of the palm), including the amplitude of the motor-evoked potential (MEP) as well as the motor map area, volume, and center of gravity to evaluate if long-term musical training and chronic pain has shrunken or enlarged the area of the brain that controls the first dorsal interosseous. The motor-evoked potential is the electrical response recorded through muscular electromyography following direct stimulation of the brain’s motor cortex; measuring the MEP provides insights into the excitability and integrity of the motor pathways.
The findings revealed that years of musical practice lead to significant adaptive plasticity and
specialized functional organization in the motor cortex. Remarkably, the presence of chronic pain did
not appear to significantly interfere with these beneficial adaptations in musicians. In other words,
even when experiencing persistent pain, musicians maintained the positive corticomotor changes
associated with their extensive training, suggesting that musical practice may build resilience against
pain-related alterations in the brain
Extensive sensorimotor training predetermines central pain changes during the development of prolonged muscle pain (Zamorano et al, 2023)
This study set out to explore the influence of sensorimotor training on the central processing of pain. Nineteen healthy musicians and twenty healthy non-musicians participated in three sessions over the course of one week. During these sessions, researchers recorded brain responses to electrical stimulation and measured pain thresholds both before and after inducing prolonged muscle pain. Prolonged pain was elicited by administering an injection of nerve growth factor into the hand.
The findings revealed several intriguing points. First, musicians reported experiencing less overall pain than their non-musician counterpartso the nerve growth factor pain over the course of the intervention. Despite this apparent resilience, musicians also exhibited heightened sensitivity to secondary hyperalgesia when lower amounts of electrical stimulation caused pain compared to non-musicians. Musicians demonstrated an increased pain response to stimuli that would not normally be painful. Furthermore, among the musicians, those who engaged in more extensive weekly training reported even lower pain scores over the duration of the study.

Experience-dependent neuroplasticity in trained musicians modulates the effects of chronic pain on insula-based networks – A resting-state fMRI study (Zamorano et al, 2019).
This study investigates how chronic pain and extensive musical training interact to influence the brain’s insular connectivity. The insula (see orange boxes in figure 3) connects various sections of the brain and modulates multisensory inputs including pain processing. Researchers used resting-state functional magnetic resonance imagery to examine the connections within the insula. The participants were split into four groups across different groups: healthy musicians, chronic pain musicians, healthy non-musicians and chronic pain non-musicians. One major limitation in this study is that the participant pool was composed of only women. People with higher insular connectivity tend to experience bodily sensations, including pain, more intensely; while those with lower connectivity may perceive these signals more mutedly, resulting in less intense pain experiences.
The findings revealed a fascinating pattern. Increased insular connectivity, observed in healthy musicians, was also displayed by non-musicians experiencing chronic pain. In contrast, musicians with chronic pain exhibited the lowest levels of insular connectivity among all groups. This suggests that while musical training may generally enhance connectivity; chronic pain, for better and worse, is correlative of changes that may suppress the perception of pain. However, as stated earlier, the population of only women in this study limits its applicability to those male musicians and non-musicians.

Pain sensitivity and tactile spatial acuity are altered in healthy musicians as in chronic pain patients (Zamorano et al, 2015).
This study explored the relationship between pain sensitivity, tactile spatial acuity, and musical training by comparing four groups: professional musicians with chronic pain, pain-free musicians, non-musicians with chronic pain, and pain-free non-musicians. Participants were evaluated for their ability to discern fine tactile details and for thresholds for thermal and pressure pain.
The findings revealed that even pain-free musicians displayed greater touch sensitivity and heightened pain responses to pressure and heat when compared to pain-free non-musicians. In addition, both musicians and non-musicians experiencing chronic pain showed increased tactile sensitivity alongside elevated pain responses relative to their pain-free counterparts. These results suggest that repetitive movements required in classical music performance might lead to changes in somatosensory pathways thus increasing the likelihood of developing chronic pain if left unchecked.
Conclusion and implications for practice
The main purpose of this blog is to educate musicians’ intuition and pain-risk assessment as musicianship may well alter pain perception. From these studies, we’ve seen findings that suggest that musicians are less, more, and equally sensitive to pain. I’ve included these methodological caveats for you to situate yourself in these findings; as generalizing these would not be wholly conclusive of individual differences and specific circumstances. In conversing with fellow musicians with similar educational background and training ages, I find that some are more resilient to pain, some are more averse to pain – for good reason. Some are more protective of their body as any pain might quickly spiral into injury; some are more willing to tolerate pain and discomfort as it is just a byproduct of the learning process. The association presented by the papers go all three ways, healthy and chronically pained musicians are more, less, and equally receptive to pain depending upon circumstances. In either cases, reduced pain awareness may support concentration during practice and performance, but it could lead to overlooking injuries developing underneath the ignorance of pain that can threaten long-term health.
As an instrumentalist and teacher, an important aspect to keep in mind in the initial appearance of pain is to discern whether it is coming from novelty (practicing something new), misuse (forcing the body to positions that it is not able to), and overuse (forcing the body to work much more than it is capable of). Much like our frog friends, it is requires careful judgment of the situation whether or not to stay in pot of boiling water, or to jump out; tolerate the pain in hoping it’s a temporary circumstance, or find different ways of playing and practice our music that causes less or no pain. Processing and being attentive to feedback from our own senses, video recordings, or trusted individuals is necessary to discern between these three points to make sense of our experience of pain to tolerate or act upon it.
References:
Kuppens, K., Struyf, F., Nijs, J., Cras, P., Fransen, E., Hermans, L., Meeus, M., & Roussel, N. (2016). Exercise- and stress-induced hypoalgesia in musicians with and without shoulder pain: A randomized controlled crossover study. Pain Physician, 19(2), 59–68. 10.36076/ppj/2016.19.59
Linari-Melfi, M., Cantarero-Villanueva, I., Fernández-Lao, C., Fernández-de-las-Peñas, C., Guisado-Barrilao, R., & Arroyo-Morales, M. (2011). Analysis of deep tissue hypersensitivity to pressure pain in professional pianists with insidious mechanical neck pain. BMC Musculoskeletal Disorders, 12, 268. https://doi.org/10.1186/1471-2474-12-26
Steeds, C. E. (2013). The anatomy and physiology of pain. Surgery (Oxford), 31(2), 49–53. https://doi.org/10.1016/j.mpsur.2012.11.005
Zamorano, A. M., De Martino, E., Insausti-Delgado, A., Vuust, P., Flor, H., & Graven-Nielsen, T. (2024). Impact of chronic pain on use-dependent plasticity: Corticomotor excitability and motor representation in musicians with and without pain. Brain Topography, 37(5), 874–880. https://doi.org/10.1007/s10548-023-01031-1
Zamorano, A. M., Kleber, B., Arguissain, F., Boudreau, S., Vuust, P., Flor, H., & Graven-Nielsen, T. (2023). Extensive sensorimotor training predetermines central pain changes during the development of prolonged muscle pain. The Journal of Pain, 24(6), 1039–1055. https://doi.org/10.1016/j.jpain.2023.01.01
Zamorano, A. M., Montoya, P., Cifre, I., Vuust, P., Riquelme, I., & Kleber, B. (2019). Experience-dependent neuroplasticity in trained musicians modulates the effects of chronic pain on insula-based networks – A resting-state fMRI study. NeuroImage, 202. https://doi.org/10.1016/j.neuroimage.2019.116103
Zamorano, A. M., Riquelme, I., Kleber, B., Altenmüller, E., Hatem, S. M., & Montoya, P. (2015). Pain sensitivity and tactile spatial acuity are altered in healthy musicians as in chronic pain patients. Frontiers in Human Neuroscience, 8. https://doi.org/10.3389/fnhum.2014.01016